
Phase One: Preparatory Work
Preparatory Work
Early on in the process of reviewing, it’s worth considering a few key issues that can inform the work you may do.
First is how to resource the project. Reviews are best undertaken with dedicated analyst time, which is often most easily accessed through NHS Public Health, but ADPs may be able to support the review too. Analysts, as noted before, can be Public Health Analysts, Registrars or ADP team members experienced in quality review, or other roles with experience in systematic analysis from case files.
The amount of file analysis time required varies, but with adequate planning and discussion with relevant parties, it can be agreed to dedicate two or three days per month of an analyst’s time to the work over the course of the review, to examine case files. If using a cohort study (see the cohort study section for more information under Phase 3), files for the largest areas may be prioritised for the analyst’s input, with additional support from the data group to undertake study in other areas.
AFS recommends that discussions between Public Health and ADP partners begin early, so that shared interests and possible resources can be identified from the outset.
Analyst, or researcher time, is not an absolute necessity for conducting a review, though it almost guarantees a quicker, easier process for all involved and reduces the timetable for review by months or years. There have been reviews in the past that have not used dedicated analyst time, but these have taken substantially longer than 12 months to complete and those who were involved strongly suggest that dedicated resourcing would be necessary.
If analyst time is not available, reviews may also be undertaken by groups of staff, with members contributing time to the process as available. This has been done in the past, though it requires careful planning and we would recommend having a lead member, or two, who can liaise with AFS to help steer the process.
A second consideration is the time of year for scheduling the phases of the review.
Some NHS boards are able to provide updates on deaths throughout the year, others are not. NRS usually release alcohol deaths data in June each year, and in some areas this is the point at which data on individual cases can begin to be analysed. Data may also be obtained from Public Health Scotland’s Data and Intelligence team (previously ISD).
When you have discussed the idea with colleagues it is worth formally approaching other ADP and Public Health partners to see how it can fit in with existing work, or could be appropriately scheduled.
AFS can offer in-person support at crucial points to ADP and Public Health teams undertaking alcohol death reviews. First in attending early project meetings to help frame the issue by providing information about alcohol deaths and how they relate to other areas of work, and give an overview of much of the detail of this guidance.
Then as the project continues AFS facilitate the Alcohol Death Researcher Network, a resource for researchers involved in projects. We can also help answer questions or put your team in contact with people around Scotland whose experience may be of use if you encounter problems. This can extend to any specificities your alcohol death review may have.
Levels of Review
Completing an alcohol death review can understandably feel overwhelming when services are already stretched. An important finding from reviews carried out so far however, highlights that there can be varying ‘levels’ of review, all of which provide valuable and important findings and recommendations.
While some reviews focus solely on alcohol-specific deaths, others cover alcohol-related deaths. For the latter, cases are often selected using the following definition of an alcohol-related death as defined by the NRS:
‘...only includes those causes regarded as being most directly due to alcohol consumption, as shown below. The definition includes all deaths from chronic liver disease and cirrhosis (excluding biliary cirrhosis), even when alcohol is not specifically mentioned on the death certificate. Apart from deaths due to poisoning with alcohol (accidental, intentional or undetermined), this definition excludes any other external causes of death, such as road traffic and other accidents. The definition allows for consistent comparisons over time for those deaths most clearly associated with alcohol consumption.’
Examples of different ‘levels’ of review include:
Example 1. A retrospective cohort review of service pathways for alcohol-specific deaths in residents of the locality registered in a three-year period.
Example 2. A retrospective cohort review of all deaths over one year, identified as alcohol-specific. A case note review was undertaken.
Example 3. A representative sample of the total number of alcohol-specific deaths in one year were reviewed, stratified by age and gender.
Example 4. While the service is unable to carry out an in-depth review, they discuss and review the alcohol-specific deaths which have occurred over the past year within their ‘Alcohol Harms Subgroup’, considering areas of learning.
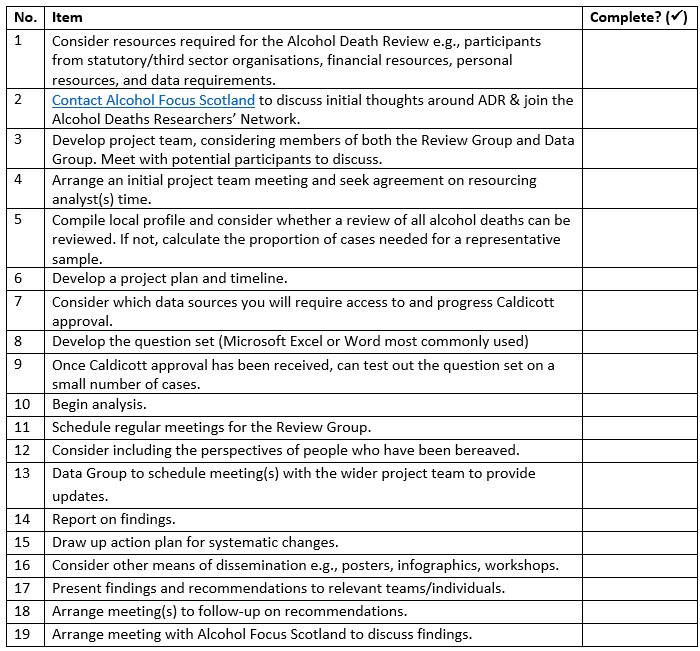
Researcher Checklist
This checklist is designed to guide reviewers systematically through the alcohol death review process, ensuring that all necessary steps are completed and key information is gathered. Use it to track your progress, maintain consistency across reviews, and ensure nothing is overlooked as you work through data collection, analysis, and reporting.
Considering Data Sources
Prior to commencing the review, it is helpful to consider the sources that you will require access to in order to retrieve case files. Case reviews typically involve study of files from more than one setting, to generate the most complete picture possible of an individual’s life (see Phase Three for further information). Typical data sources include:
-
GP case notes
-
Other Primary Care records
-
Hospital records
-
Other inpatient and outpatient notes
-
Community Addiction Team case notes
-
Community Pharmacy notes
-
Cancer Registrations
-
Third Sector notes
-
Social Work records
-
Housing records
-
Police and Fire Service records
NHS Primary Care patient records are typically held post-mortem, in hard copy, at local Practitioner Services facilities, often the same site already known to drug deaths researchers. Access to these records can require in-person attendance as files cannot leave the premises. Some teams were able to access electronic files by contacting individual GP surgeries for case notes; they were provided with a login for either Vision or EEMIS after they signed a confidentiality agreement. Others received electronic primary care records from NHS National Services Scotland. They described this as a simple process, where the NSS downloaded the patient information to Global Scope and provided a login. To find out more, email: nss.psdenquiries-general@nhs.scot
NHS Acute Records are held in different places across different sites. In some areas they are held centrally post-mortem, in others they are kept in hospitals. In either case, having an effective working relationship with staff at various sites is crucial in facilitating access to records. Having clinical input, from nurses and doctors directly involved in treatment, on the review and/or data group can assist with this process. Some areas have e-health programmes that can facilitate access to this data.
Some teams have utilised record linkage undertaken for the Patient Level Information Costing System (PLICS) dataset developed by Information Services Division (ISD) Scotland. The PLICS dataset links together patient level information collected from the following national data schemes:
-
General acute inpatient and day case hospital admissions - Scottish Morbidity Record (SMR) 01
-
Mental health inpatient and day case hospital admissions - SMR04
-
Outpatient clinic appointments - SMR00
-
Emergency department attendances - A&E2 datasmart
-
Community pharmacy prescribing - Prescribing Information System (PIS)
Additional sources of data for alcohol death reviews may also come from:
-
The Clinical Portal for Community Pharmacy notes - contact details for each NHS Board can be found here: www.communitypharmacy.scot.nhs.uk/contact-us/
-
PiMS
-
Genisys
-
CareFirst
-
Data is transferred to a central repository 3 years after the individual’s death. Some ADPs have highlighted that it can be simpler to request data after this time. Further information can be found at the NHS Central Register - National Records of Scotland (NRS)
Social Work Records are held by local authorities. There is no national social work database, and record availability, electronically or on paper, varies by area. It is worth consulting with social work colleagues on your review group to find out how best to link the data – typically a CHI number or NI number is most helpful, both of which should feature in NHS data. Access to these records, if they are held physically, typically involves visiting an archive.
Third Sector Records are often held electronically, and may be accessible under data-sharing agreements described as part of the service contract if commissioned through an ADP or Health and Social Care Partnership (HSCP.) For services not commissioned through an ADP, for example an independent treatment service, it is worth considering inviting someone from that organisation to the review group and establishing a data sharing agreement for the purposes of the review, which can satisfy Caldicott guidelines.
Other Statutory Records including housing, police records and others. As local data sharing agreements vary, and points of contact are crucial, we advise considering how to involve these sources early in project planning, so contacts can be made if needed.
In this section
- Policy reports
- Research
- Briefings
- Practical guides
- Alcohol Deaths Review Guidance
- Ministerial Foreword
- Introduction
- Phase One: Preparatory Work
- Phase Two: Establishing the Team
- Phase Three: Planning the Review
- Phase Four: Undertaking Research
- Phase Five: Preparing and Disseminating Findings
- Factsheets
- Consultations
- Manifesto
- Corporate documents
