
Introduction
This guidance is intended for use by Alcohol and Drug Partnerships (ADPs) and NHS Public Health teams concerned with alcohol deaths prevention. It is intended to be used as a reference manual for teams at any stage of planning alcohol death reviews, from initial consideration through to publication.
The guidance has drawn on best practice from those who have previously completed Alcohol Death Reviews. Conversations with stakeholders from ADPs across Scotland sought to find what had worked well, what could be learned from and what people would do differently if their reviews were repeated. We are grateful to all those who shared their experience and reflections to contribute to the project.
The sections of the guidance mirror the practical concerns and thinking to be done at all stages of review. We are aware that local teams have varying priorities, interests and resources, and so we have developed this guidance to give a general overview of how alcohol death reviews can be carried out, leaving space for ADPs and NHS Public Health teams to develop their own reviews as they see fit.
This guidance forms one element of AFS’s support for teams concerned with alcohol deaths prevention, alongside the Alcohol Deaths Researchers’ Network and ongoing project support available from the AFS team, as reviews are planned and undertaken.
For further information or support on alcohol deaths prevention please contact Catherine White at catherine.white@alcohol-focus-scotland.org.uk.
To view the content of this section, click through the boxes below.
What are Alcohol Death Reviews?
Reviews of alcohol deaths study information about a person’s life, and death, in order to evaluate what opportunities could be taken in future to prevent other people dying in similar ways.
Reviews of alcohol deaths involve gathering qualitative information to understand how alcohol played a role in a person’s life and eventual death. Reviews can draw on GP records, notes from acute treatment, third sector organisations and the recollections of families.
How can reviews help?
One of the major obstacles to preventing alcohol deaths in Scotland today is a lack of knowledge about how services might help people at risk of dying by alcohol, and the course of addiction through people’s lives before they die. Annual National Records of Scotland (NRS) statistical information is available, but little else is reported at the local or service level.
Core Aims and the Review Process
Core Aims of Alcohol Death Reviews
Across the reviews completed to date, three fundamental aims consistently emerge:
1. Understanding Patient Journeys and Service Engagement
- Investigating trends over time and variations by gender, age, deprivation, and geographical area
- Identifying patterns of engagement with services and where they break down
- Assessing service pathways and the effectiveness and impact of services
2. Identifying Key Risk Factors
- Analysing risk factors emerging from comprehensive data analysis
- Understanding the complex interplay of social, health, and personal factors contributing to alcohol-related deaths
3. Generating Learning Points for System Improvement
- Informing potential early interventions to prevent alcohol-related deaths
- Developing effective support for end-of-life care
- Identifying areas for priority action and strengthening multi-agency awareness
- Improving population-level outcomes through evidence-based recommendations
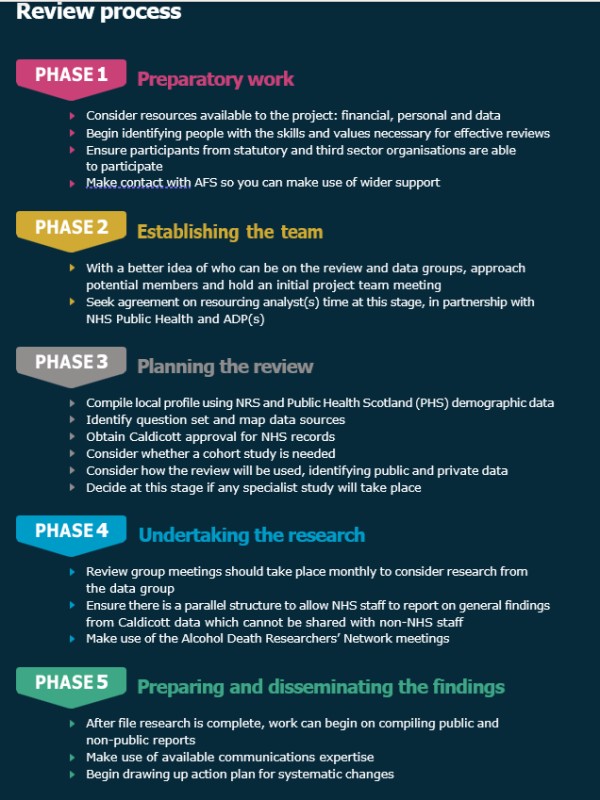
There are generally five phases to the review process (see below). This guidance provides detailed advice and templates to support at each stage of the review.
Alcohol Deaths Researchers Network
Alongside the guidance, Alcohol Focus Scotland has established the Alcohol Deaths Researchers’ Network (ADRN) to facilitate communication, support, and information sharing between people involved in reviews. This network currently meets quarterly and welcomes active and former researchers or analysts from across Scotland.
The ADRN serves as a vital platform for knowledge exchange, enabling practitioners to share experiences, discuss challenges, and develop best practices in alcohol death review methodology. The network addresses the isolation that individual teams might otherwise experience when undertaking these complex and sensitive reviews. The collaborative approach fostered by the ADRN ensures that lessons learned from individual reviews contribute to improved practice across Scotland’s alcohol death review landscape.
The network represents a crucial infrastructure supporting the expansion and enhancement of alcohol death reviews across Scotland, providing both practical support and professional development opportunities for those engaged in this important work.
If you would be interested in learning more about the network, please contact: enquiries@alcohol-focus-scotland.co.uk
Values and Aims of Reviewing
Alcohol death reviews offer an opportunity to undertake open-minded work with a view to improving the health of people across the country. Given the stark inequality in alcohol mortality - people in Scotland’s most deprived communities are more than four times more likely to die than those in the most affluent communities – it also offers an opportunity to address this inequity. The people AFS have spoken with who are experienced in alcohol death reviews were unanimous in their enthusiasm for reviews, and believed they had made it possible to consider alcohol deaths in a way which was impossible before.
Having reliable data was identified as a crucial output, but so was building effective, collegial links across specialties and sectors. Though this guidance is largely technical, the values of collaboration, open-mindedness and curiosity were mentioned repeatedly by experienced reviewers as being crucial to the success of alcohol death reviews.
Every death by alcohol is a tragedy, and with AFS’s work being to assist local ADP and NHS Public Health teams in collaborating to reduce them, alcohol death reviews have a specific place in quality and service improvement. Reviews aim to evaluate and improve the coverage and provision of support for people at risk of dying by alcohol. They should achieve this through collaborative practice from the outset, ensuring that lessons can be learned and improvements implemented across the whole of the healthcare system, wherever a person might need support.
Alcohol-specific vs alcohol-related deaths
Often professional discussions use the general term “alcohol deaths,” but in fact there are two similar terms with different meanings, and the difference between them is critical for public health professionals.
Alcohol-specific deaths are ones which could not have occurred other than through alcohol use – these are reported by the NRS, usually in June.2 There are also annual statistics on the rate of alcohol- specific deaths published by the Office of National Statistics (ONS) every December3 and the MESAS monitoring reports in June address inequalities in relation to deaths.
Alcohol-related deaths is a broader definition. These include any death where alcohol is assessed as playing a role, not just being biologically caused by it. These can include alcohol-specific deaths plus other causes such as accidents, suicides, cancers and other physical conditions commonly linked to, but not directly caused by, alcohol use.
Alcohol-related conditions are far more numerous than alcohol-specific ones. Because of this there are usually practical decisions to be taken by researchers or analysts on which alcohol-related conditions their work will focus on. For a broad sense of the conditions which can be linked to alcohol misuse, ScotPHO’s 2018 Burden of Disease from Alcohol Consumption report is instructive. Having a clear sense of the conditions being examined will set the course for further developments in research, across the healthcare infrastructure and ultimately public health strategy. In most cases we would recommend first reviews examine alcohol-specific deaths only, but there is more guidance under Phase Three, and AFS can be contacted for support in the planning stages of a review.
Are there similarities between alcohol death reporting and drug death reporting?
People often ask about the relationship between drug and alcohol problems, treatment, deaths and recording, and what systematic differences arise between them. As a result of the many differences, the alcohol review process AFS recommends in this guidance is different to drug death reviews in many ways.
Put simply, drug deaths tend to be medical emergencies including overdose, whereas alcohol deaths tend to be the result of chronic conditions. We know from anecdotal accounts from treatment providers and researchers that alcohol-specific deaths are more likely to take place outside of specialist addictions support than is the case for drug deaths, and with alcohol deaths being less instantaneous than drug deaths the means of preventing them are liable to be very different too.
Deaths suspected of being caused by illicit drug use are classed as ‘unnatural’, triggering legal processes for investigating them. Toxicology study, and sometimes autopsy, are used to determine whether a death was related to drug use.
Alcohol deaths rarely trigger that legal process. The conditions which kill people tend to be chronic, developing over years, often with few or no physical symptoms until advanced damage has been done. While the role of drugs in deaths is assessed with toxicology study, for alcohol this is not the case. Assessing the role of alcohol in a death usually rests instead on determinations by the physician who completes the death certificate.
These differences in the nature of, and legal requirements relating to, alcohol and drug deaths have implications for the ways in which data are collected and reported for each. Alcohol’s status as a legal drug means very few alcohol-specific deaths trigger legal investigation after death.
The chronic nature of the conditions which cause deaths by alcohol mean that GP and other community-based records are of primary importance for understanding how a person lived and died.
These differences have to be kept in mind when reviewing alcohol deaths. Reviews of drug or alcohol deaths can yield similar qualitative data about a person’s life and their substance use, but there are structural differences in reporting which are important for researchers to keep in mind.
Where does data come from?
Whenever a person dies in Scotland, the death has to be registered. When this happens there are two documents issued – the first is a ‘short form’ death certificate, which can be taken away by families, and the other is the Medical Certificate of the Cause of Death form (MCCD).
The MCCD includes a primary cause of death and contributory causes, assessed by a trained physician. These causes correspond to ICD-10 codes, which are internationally-agreed, used to record illnesses and conditions throughout treatment and after death. These codes are used in the recording of alcohol deaths.
In cases of alcohol-specific deaths, ICD-10 codes recorded on the MCCD are more likely a matter of professional judgement than definitive post-mortem examination. This is due to the chronic nature of many conditions, alcohol’s legal status and other factors.
Because of this, the role of alcohol in deaths across Scotland may be subject to some inconsistencies in reporting, for example in the absence of specialist testing or care.
However, this should not affect reviews undertaken with this guidance. The aim is to get more information about the cases which are conclusively listed as alcohol-specific, or alcohol-related, within the current system.
The National Picture and ICD-10 Codes
Scotland’s rate of alcohol-specific deaths is the highest in the UK. To date however, there has been relatively little study of how people who die by alcohol interact with the services and supports that are available. In 2021, the Scottish Government rightly recognised alcohol harm as a public emergency, alongside drug deaths. Since then, alcohol specific deaths increased to a 15 year high in 2023. Most recently, there were 1,185 alcohol-specific deaths registered in Scotland in 2024, a decrease of 92 deaths from 2023 (National Records of Scotland, 2025)
At the national level roughly twice as many men die from alcohol as do women, though at the local level this can fluctuate dramatically year-on-year. Without wider data it is hard to conclusively know why this is. We know also that, in line with other alcohol harms, alcohol deaths occurred over four times more frequently in the most deprived communities than the least in 2023.
Alcohol Specific Deaths in Scotland, 1994-2024
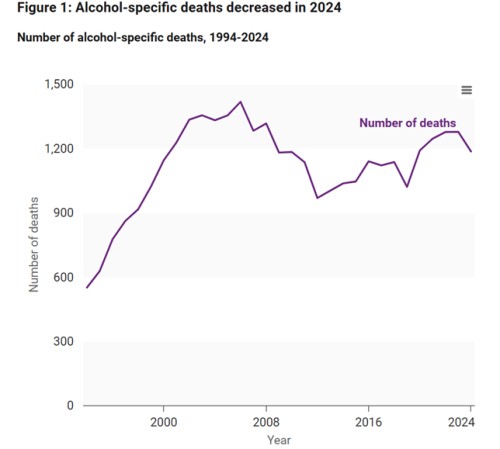
Figure 1. Source: National Records of Scotland, Alcohol-specific deaths 2024
Yet even these figures only show the tip of the iceberg; Public Health Scotland estimate that the total number of deaths caused by alcohol is likely to be more than double. The alcohol-specific statistics only capture deaths from conditions that are caused by alcohol alone, such as alcohol-related liver disease and alcohol dependence syndrome. In fact, most deaths due to alcohol are from wider alcohol-related causes, such as cancers, heart conditions, stroke, and accidental injuries. Each is a life cut tragically short and leaves behind family and friends suffering their loss.
Unfortunately, the COVID-19 pandemic and restrictions has exacerbated Scotland’s alcohol problem, with increased harmful drinking and reduced service access driving increased harm. If these changes in consumption persist into the long term, it is estimated that this will lead to around 7,500 more deaths and 70,000 more hospitalisations by 2040, costing £82.2million in hospital costs alone. Anecdotally, services report higher demand and greater complexity in cases, with people presenting in poorer health.
Recent figures reveal that access to alcohol treatment is at its lowest in a decade, with a 40% decline in the number of people starting specialist alcohol treatment from 2013/14 to 2021/22. Although the Scottish Government has tasked Public Health Scotland with investigating this decline, it is clear that there is both a failure to prevent harm and a gap in treating it.
Our alcohol problem is disproportionately felt by people living in Scotland’s most deprived communities, where individuals are over four times more likely to die due to alcohol and six times more likely to be hospitalised compared to those living in the wealthiest areas (Public Health Scotland, 2023). When harm increases, it affects these communities most severely.
While deaths are the most extreme form of alcohol harm, they are likely to be accompanied by increases in other harms which can impact those experiencing alcohol problems as well those around them. These impacts can themselves be life-changing and include alcohol-related diseases, accidents, violence, unemployment, family and relationship breakdown, domestic abuse, child neglect and fetal alcohol spectrum disorder. This is compromising people’s right to health, which the Scottish Government has a legal duty to respect, protect and fulfil. None of this is inevitable. By taking action now we can save and improve thousands of lives.
How does alcohol cause deaths?
The graph below shows the proportion of alcohol-specific deaths by some of the common ICD-10 categories in Scotland in 2023:
Causes of Death, Scotland, 2023

Figure 2. Source: NRS Alcohol-specific deaths 2023
ICD-10 codes classify medical diagnoses in a specific way. The first three characters—a letter and two numbers—classify the disease or health condition. After the ‘period’, the subsequent three numbers describe the cause of the disease, how severe it is, or where in the body it is located. Each ICD-10 code starts with a capital letter from A to Z, highlighting the nature of the condition:
A: Infectious and parasitic diseases
B: Infectious and parasitic diseases
C: Cancer
D: Neoplasms, blood, and blood-forming organs
E: Endocrine, nutritional, or metabolic
F: Mental and behavioral disorders
G: Nervous system
H: Eyes, ears, nose, and throat
I: Circulatory system
J: Respiratory system
K: Digestive system
L: Skin
M: Musculoskeletal system
N: Genitourinary system
O: Pregnancy and childbirth
P: Perinatal conditions
Q: Congenital and chromosomal abnormalities
R: Abnormal clinical and lab findings
S: Injury, poisoning, and other external causes
T: Injury, poisoning, and other external causes
U: Used for emergency designation
V: External causes of morbidity
W: External causes of morbidity
X: External causes of morbidity
Y: External causes of morbidity
Z: Factors influencing health status and contact with health services
Additional numbers and letters assist to further characterise the condition. The following conditions as coded by the ICD-10, are counted as alcohol-specific deaths in Scotland:
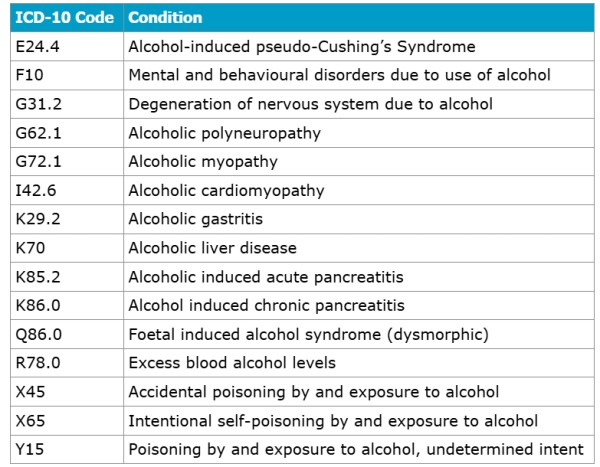
Figure 3. ICD-10 Codes
During conversations with the ADRN, concerns have been highlighted about the coding used on death certificates, with F10 deaths (mental and behavioural disorders due to use of alcohol) disproportionately high compared to the rest of the UK. This has brought the reliability of the data into question. It was highlighted that while drug-related deaths have post-mortems and toxicology data, alcohol deaths often lack such data making it challenging to piece together an accurate story.
In these instances, it can be helpful to examine the four-character codes, as these can provide more nuance when interpreted alongside the information on the death certificate:
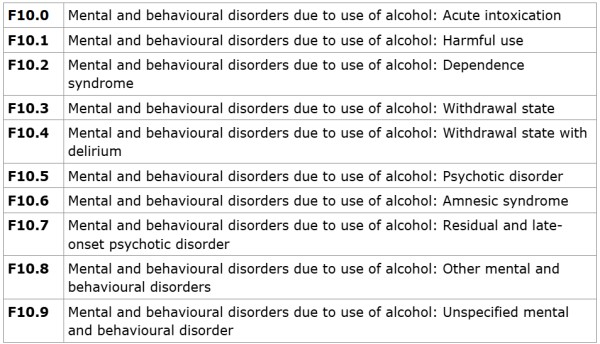
Figure 4. ICD-10, F10 Codes.
Phase of Reviewing
Previous reviews have varied widely in design and findings, but our research indicates a five phase model that can be of use to those planning future reviews. These are practical phases, which we believe can be undertaken in a 12-month period as part of a review, assuming effective planning and resources are available.
Phase 1: Preparatory work – involves initial thinking and informal discussion with possible participants in the review, as detailed later on in this guidance.
Phase 2: Establishing the team – is a more formal period with initial meetings and the active involvement of a wider group.
Phase 3: Planning the review – moves this group into a period of active planning and ensuring resources are available for the study.
Phase 4: Undertaking research – sees the study take place, with regular meetings between review and data groups.
Phase 5: Preparing and disseminating findings – sees the preparation of findings and their dissemination, with ongoing actions set with partners across the healthcare systems, including statutory and third sector groups.
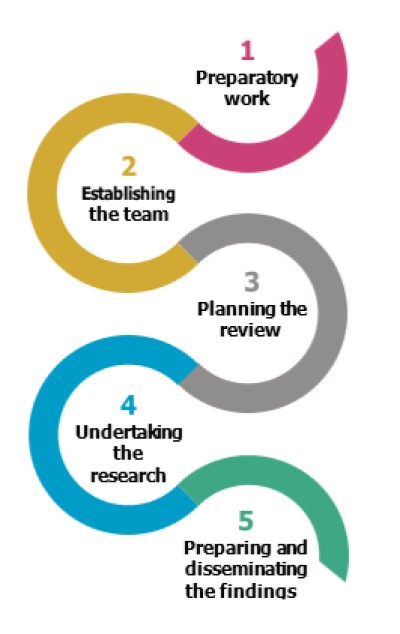
Figure 5: Phases of Alcohol Death Reviews
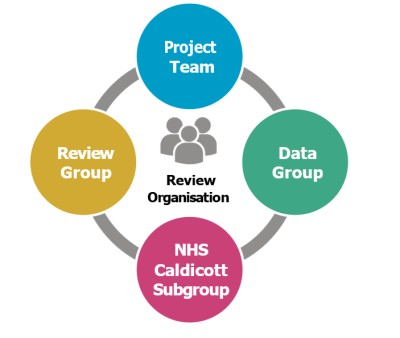
Review Organisation
For efficient organisation of the review, AFS recommends project teams consist of two groups.
-
The data group analyses files and is responsible for the technical aspects of the review.
-
The review group steers the content of the review, considers the data to generate findings and is responsible for compiling the public and private reports for publication.
More information on the NHS Caldicott Subgroup follows below.
The data group generates data for the study, from public information and individual case files. Data group members should have experience of analysing or researching patient records and may consist of Public Health Analysts, Registrars or ADP team members with experience of research or data analysis. Prior knowledge of addictions should not be a requirement for data group members. Discussion with the review group can bridge any gaps in knowledge.
The review group’s purpose is to be both a sounding board for the analysts in the data group, and to steer the study through its phases. The review group should be multidisciplinary and have a longer-term view of the study and its use. Members of the review group should be people from across treatment levels, both statutory and third sector, with the power to make changes recommended by the review. The review group should also include named responsible figures for the Caldicott application.
Sometimes there may be members of the project team who are part of both groups. For example there may be ADP staff whose analytic skills are useful in the data group, but who can also provide input on community addiction support systems through the review group.
Due to regulations around confidentiality and data handling, all members of the project team will have to be staff members employed within a statutory or third sector organisation.
Because of the requirement that personal NHS data is analysed only by NHS staff (see Phase Three for more on Caldicott processes), there is a requirement to have an NHS Caldicott subgroup which involves NHS staff from the review and data groups. This subgroup can then analyse Caldicott-sensitive sources and present aggregated information about interaction with NHS services for use in the final reports.
As part of the research towards this guidance, AFS also examined how lived and living experience can be involved in alcohol death reviews. To our knowledge, there have been no alcohol death reviews carried out in Scotland which have involved family members or loved ones. To involve those with lived experience however, could happen in a couple of different ways.
First is involving people with a connection to someone whose files are examined in the review. To date this has not been a feature of any of the alcohol death reviews we know of, but there are examples of practice in other areas such as drug deaths reviews and suicide reviews. We consulted bereavement support specialists who advised that the process of recollecting a person’s life can be beneficial for people who have lost someone; it can also be acutely difficult for those involved. More information is available under Phase Four.
The second means of involving lived or living experience is in service design and improvement, which AFS actively encourages review groups to do as part of their action planning. This can be helped by involving recovery services throughout the review process, and by making sure there is time and practical support to involve people with lived experience as action plans are generated. More information is included under Phase Five.
In this section
- Policy reports
- Research
- Briefings
- Practical guides
- Alcohol Deaths Review Guidance
- Ministerial Foreword
- Introduction
- Phase One: Preparatory Work
- Phase Two: Establishing the Team
- Phase Three: Planning the Review
- Phase Four: Undertaking Research
- Phase Five: Preparing and Disseminating Findings
- Factsheets
- Consultations
- Manifesto
- Corporate documents
