
Phase Three: Planning the Review
Data Sources
Case reviews can draw upon a number of data sources to assess how support for people at risk of dying can be improved through a range of settings and interventions. As previously discussed, National Records of Scotland (NRS) publish annual statistics on alcohol-specific deaths in June. This publication details the number of deaths across Scotland, broken down by health board/local authority area, age and sex.
This data, plus information provided by each area’s Local Intelligence Support Team (LIST), from Public Health Scotland can be used to generate a local profile of alcohol deaths. LISTs can provide a range of personal data for cases which can be useful in building a local profile. ADPs have highlighted the value of gathering local data, where this can often be more impactful when presenting data and findings to decision-makers.
The second stage of alcohol death reviews is the case review, where individual case files are analysed to understand the circumstances of people whose deaths have been caused by alcohol. NHS Health Boards collect data on all deaths, organised by ICD-10 code, every week. This data may be used on a rolling basis through the year, but carries a risk of missing some deaths: as unascertained causes are not included in those releases, the NRS data in June is the most comprehensive available for the whole-year period.
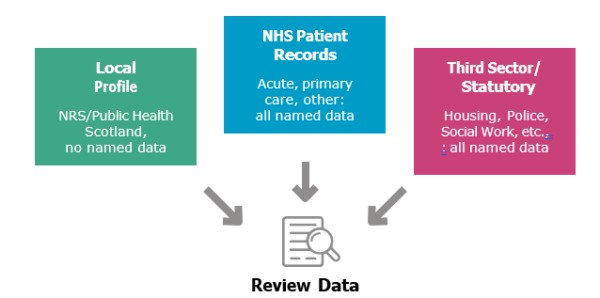
Case reviews typically involve study of files from more than one setting, as discussed under Phase One. The reviews completed to date have utilised diverse data sources including:
- GP case notes
- Addiction team records
- Clinical portals
- Electronic health records
- Social work records
- National datasets (Scottish Morbidity Records, Prescribing Information System, A&E2 Datamart)
- Information from third sector organisations.
Some reviews employed comprehensive record linkage methodologies, while others focused on targeted case note analysis or specific service pathway examination. Of course, ensuring access to these records requires a degree of planning. This is covered later on in this guidance, but we recommend planning not just for the study areas, but the permissions required and how these can be obtained. ADPs may play a role in working with commissioned services, and should examine their data-sharing protocols as necessary. Doing this well in advance of seeking Caldicott permissions helps ensure that process runs smoothly, allowing the study to proceed as quickly and efficiently as possible.
Local profiles
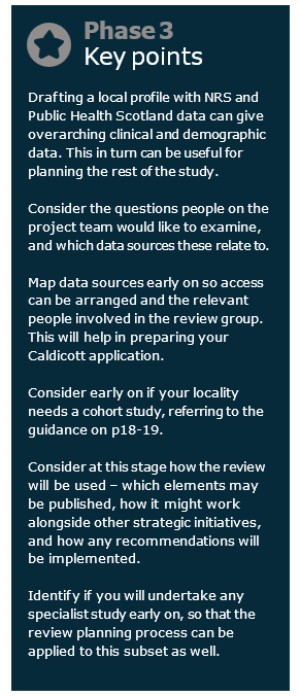
Local profiles give demographic context to the overall problem of alcohol deaths. Having a sense of the gender split, age, ethnic background and service interaction can be useful in shaping the cohort and identifying particular areas for study.
Local profiles of alcohol deaths can be generated using data from NRS, which can be broken down to health board or local authority level, and Public Health Scotland. This is not named patient data, and so requires no specific Caldicott approval; it can be undertaken in parallel with seeking Caldicott approval for the case review.
The local profile can be a useful first part of the review report, giving context of your local area(s) with reference to the rest of Scotland and/or other parts of the UK with similar socioeconomic profiles.
If your area already generates an annual alcohol profile then it could be helpful to include data from the alcohol death local profile in this, even in years where you are not conducting a full case review.
Templates for Data Collection
Establishing a Cohort
An in-depth analysis of a representative sample of cases may be conducted if the total number of cases is too high to be examined in full. While case reviews are always useful, deciding whether or not to use a representative sample is a matter for the teams in each area.
AFS advises that project teams refer to the number of deaths in ADP areas when deciding on whether or not to use a sample. Because ADP areas correlate with local authority areas, determining cohorts at this level allows results to easily link with support from statutory local authority and third sector services.
Cohort studies need to analyse 30-50% of cases in the area in the year of study, based on experience in previous reviews. With AFS’s research showing that a dedicated analyst’s time should allow analysis of 50-60 files over several months, towards a total review time of 12-16 months, this can be used to assess whether or not a cohort may be used in an area.
-
If an ADP area has fewer than 50 deaths it should be able to analyse all the alcohol-specific deaths that year with dedicated analyst time.
-
If an ADP area has more than 50 deaths it may be necessary to use a cohort of 30-50% of death cases in that ADP area, and analyst(s) time should be considered accordingly.
-
For example, you might review 50% of 86 cases (43 cases); 40% of 120 cases (48 cases); 30% of 180 cases (54 cases).
Establishing a cohort
Cohorts should be representative of the general population who died in the area. Look at the NRS and Public Health Scotland data for your area in the year of study and evaluate:
-
Age at death;
-
Sex;
-
Race and ethnicity;
-
Level of deprivation (Scottish Index of Multiple Deprivation (SIMD) of home address).
The cohort demographics should mirror, as closely as possible, the demographics for the total population who died in the year of study. Coding named person data for demographics can help this process. SIMD data can be accessed for known postcodes, across a number of deprivation domains.
There may be other factors that influence individual cases’ inclusion in the cohort, for example, availability of data; if it is not possible to access GP patient records, or if the review group believes that accessing notes from acute hospital admissions would be prohibitively difficult, there may be grounds to exclude individual cases.
If this decision is taken, we would encourage the review group to raise the issue in discussions with AFS, so as to identify gaps in our knowledge at the national level and possible areas for future study.
Time Needed for Case Reviews
Proper time needs to be given to consider the findings from case files. The review and data groups should collectively discuss the areas for study and identify specific data items for examination in files.
With sufficient resources in place, it should be possible to complete a review in 12-16 months, with approximately:
-
4 months planning the project,
-
6 months undertaking the research,
-
2 months compiling and considering the final report.
Experienced researchers suggest that with sufficient planning and a useful question set, they can analyse the NHS primary care and acute records of 3-4 patients per day. This can then be supplemented with information provided by third sector and other statutory partners as requested in a batch at the start of the research period.
Caldicott Approval
Obtaining Caldicott approval has been identified as the single biggest hurdle before starting the research for many reviews in the past. Having an early discussion with someone in the Caldicott office can help, as can having the time of an experienced researcher in the data group, and ensuring you involve people from relevant data sources involved in the process early on.
Caldicott permission is an essential part of the review process, and can be helped by enlisting the support of an experienced researcher or analyst, and planning applications early.
Some of the information used in reviews is publicly available, and therefore requires no Caldicott approval. NRS data is public, and needs no approval to form part of a review. “Named Person” data for the case file study will require Caldicott approval however, to ensure patient confidentiality is protected.
Named person data identifies the particular details of a person’s individual case. Patient records along with files from other settings, all count as named person data.
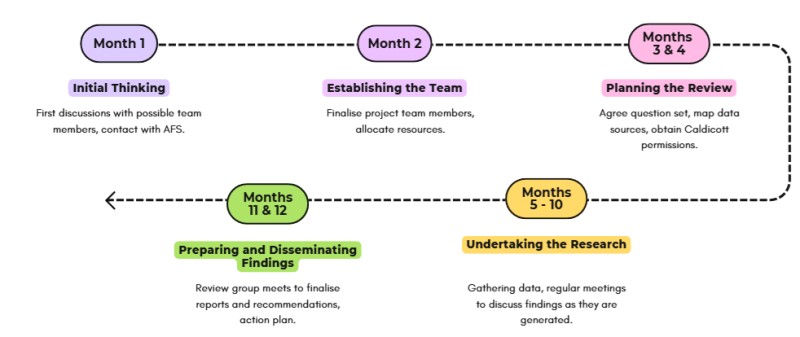
Figure 1. Timeline of Review Process
Caldicott Approval
Using NHS-held named person data requires approval under Caldicott information sharing protocols. Requests are reviewed by the Caldicott Guardian for each NHS Health Board, with requests typically considered at a regular monthly meeting. More information about the NHS Scotland Caldicott processes can be found through your local Caldicott Guardian.
If your study has input from public health researchers it is likely they can help guide this process. In some cases Caldicott Guardians have existing links with other figures in public health, which can help to smooth the process significantly.
Caldicott applications detail the data being requested, how it will be stored, the arrangements for sharing it with any partner organisations, and the reasons for approving the request under the Caldicott principles.
It is important to prepare an application carefully, after planning what data will be requested, so that the process can be as smooth as possible. Itemising the data points as other reviews have will help with this process (this is covered in the next section).
It is helpful to consider a publication plan ahead of submitting Caldicott approval, as there may be implications if named person data were to be published, even in anonymised format (for example where numbers are small enough to enable individuals to be identified).
Caldicott meetings vary by area but it can take anywhere between several weeks and several months to clear the process. Make sure you contact the relevant Caldicott Guardian for your area early in the process to make them aware of the planned research and ask for any guidance they can offer in preparing your application.
Caldicott approval lasts for a certain period you apply for, and so your review could be ‘timed out’ if it overruns. This is not necessarily, in practice, a major problem but can be avoided by having a considered timescale for the work, factoring in resources available and planning for contingencies. If there is an overrun it should be possible to request an extension in good time, and this should be considered sooner rather than later if it seems like it may be necessary.
Research Plan
Having a research plan can be a significant help in establishing clear timescales for the project and ensuring the relationship between review and data groups is clear from the outset. We recommend reviewing files on a rolling basis, with monthly or bimonthly meetings of the review group to consider data as it becomes available, in the form of key updates from case files.
Consistently reviewing files gives the review group an opportunity to get a sense of any issues as they become apparent, and to become familiar with the project’s output ahead of compiling and responding to the report. We have no specific recommendation on how often the review and data groups should meet while the research is taking place, though some interviewees suggested that at least once during the process would be helpful. Instead the review group can continue to consider findings prepared by analysts from the data group on a monthly basis.
A research plan can also help in ensuring the work remains on-track. As individual patient records vary substantially in size, it is possible to check early on in the process whether or not the timescales may have to be adapted. This can free up review group time, and allow the project to continue without becoming onerous for those involved. Similarly, a research plan allows the data group to check their progress and identify possible issues ahead of time.
Social work, police and other statutory records
Local arrangements for data sharing should be examined early on in planning, and consulted in cases where data from other statutory records are sought. Given the specific nature of alcohol death reviews it is unlikely that workers from non-addictions settings would be interested in attending every review meeting. Therefore consideration should be given at an early stage as to how to obtain data as easily as possible and allow for timely input from other agencies as findings are considered.
Third sector records
Including third sector records in review studies is extremely valuable, given the significant role third sector agencies play in facilitating recovery and avoiding death. If it is possible to include third sector treatment providers in the review group this would be especially helpful; these representatives can help facilitate access to records for the purpose of the review, in line with General Data Protection Regulation (GDPR) and other data- sharing protocols. These may already be in place under ADP commissioning protocols.
Ensuring your review group includes senior representatives from commissioned third sector services, statutory agencies and other settings whose data will be used in the review can be an enormous help in obtaining Caldicott approval and planning the study. In turn it can help to ensure findings are publicised and implemented.
Establishing and Testing the Question Set
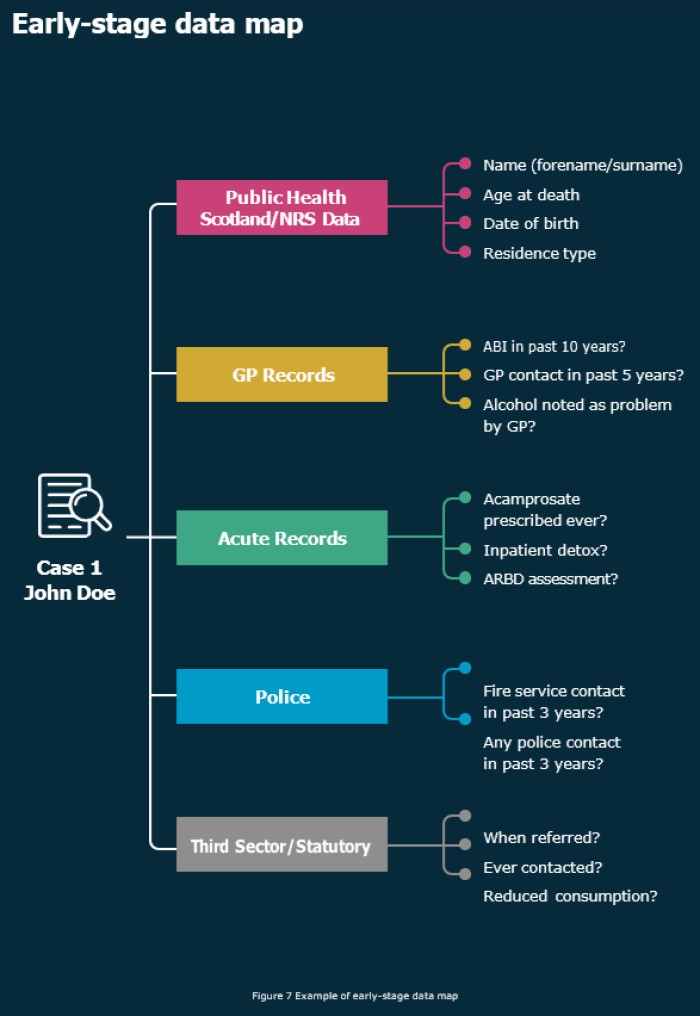
The project team should work collectively to take areas of concern and map them against data items, before turning this into a question set that can be used by researchers or analysts to analyse individual files. In some areas, question sets have been derived from sources including other research on alcohol-related deaths, and questions used for drug-related deaths. Templates which have been used in other areas are available for you to download and adapt for use at the bottom of this page.
Beginning with a map of data items and sources can be helpful (see above). A data map can then be turned into a question set, to allow data on cases to be collected across different settings more efficiently. For example, a question set for required data from third sector sources could be developed so that when a case is shown to have contact, this can be sent through the relevant service manager on the review group to that service, who can quickly gather the information.
It is helpful to categorise data items in broader categories. Criteria which has been analysed in previous reviews includes:
-
Demographics
-
Alcohol problem and history (this includes items such as units consumed, type of alcohol, age the individual was when they first consumed alcohol drank, age when they first sought support)
-
Contact with alcohol services
-
ABI screening
-
Health and contact with acute services
-
Alcohol relapse prevention medication and vitamins
-
Alcohol detox
-
Liver transplant
-
Other substances
-
Services referred to and attended (primary care, secondary care, inpatient, outpatient, emergency services)
-
Physical health conditions
-
Mental health conditions
-
Social issues
-
GP contact
-
Police contact
-
Fire Service contact
-
Other Social Work contacts
-
Third Sector support
-
Clinical Portal (letters, appointments)
-
Themes identified throughout
If your review includes third sector files, treatment for alcohol-related illnesses, ARBD or focuses on other demographic groups, it would be useful to itemise these data within separate categories.
Testing the question set
Trialling your question set on a limited number of files can be useful, especially in areas using a cohort study because of high numbers of deaths. Any gaps in data or other issues can be addressed through this pilot study, acting as a ‘dress rehearsal’ for the full review process, including seeking Caldicott approval and familiarisation with the research processes for new researchers.
Findings from files in the pilot can still contribute to the overall review, but allow problems to be identified early in the process. Typically a pilot covering 20% of the cases to be covered in the cohort study is sufficient to resolve any issues. These results can be analysed by the review group as well, giving a sense of the way meetings can be carried out in future.
Specialist Studies
While this guidance gives an overview of how to undertake reviews of alcohol deaths, some areas may want to undertake specialist study of an area of particular interest or concern to local partners. These may include, but are not limited to: alcohol-related deaths; cases related to particular pathways such as ARBD or community detox; or cases from particular demographics.
Undertaking specialist studies within a review is by no means necessary, but can add weight to local understanding of particular issues. In practical terms, the process of special studies is no different to the usual review process; these practices would just be applied to a specific category of cases, perhaps as a sub-cohort.
If in doubt as to whether or not to undertake a specialist study, AFS recommends focusing on a general review for the first study, as specialist studies can be undertaken in more depth in the future with more experience to guide them.
We recommend that review groups consider any specialist study at the earliest stages of planning, as research planning and ethics processes need to take account of the specialist study’s needs.
AFS’s research indicates that ADPs or Health Boards with access to one researcher for the project can expect to review 50-60 case files in depth, supplemented by additional data from third sector and other statutory records. In ADPs or Health Boards with fewer deaths, there may be interest in reviewing files where the cause of death is alcohol-related, not just alcohol-specific.
Special studies can be considered from the earliest stages of planning and work on the local profile. This can allow for different ICD- 10 codes to be gathered, for example those accounting for alcohol-related deaths under the ScotPHO definition laid out in the 2018 Burden of Disease Attributable to Alcohol Consumption report,11 or cases of suicide (codes X60-X84).12
Given the much broader scope of alcohol- related deaths, both in terms of medical specialty and numbers – with about four times as many alcohol-related deaths as specific – it is important to be clear on what would be studied in your area, if you choose to pursue a study of alcohol-related deaths.
ScotPHO’s 2018 Burden of Disease study can be instructive here. There are 30 alcohol-related conditions detailed in this report, under categories that can guide project teams’ thinking such as “malignant neoplasms” (cancers), “cardiovascular disease,” and injuries both intentional and unintentional. These kinds of special studies, alongside a full review of alcohol-specific deaths, can help bring an alcohol focus to other elements of public health work, for example suicide reviews or heart disease.
Having identified the causes of death you would like to include in the review, the ICD-10 codes listed in the ScotPHO report can be used in a process parallel with the main review, using the same methodology described in this guidance.
It can be useful to identify at an early stage how the caseload of a specialist study would fit with the main report into alcohol- specific deaths. For example if two analysts are required to evaluate the combined 90 case files required for the alcohol-specific review, but their combined capacity is closer to 100-120 files, it may be possible to undertake a specialist study of 10-30 alcohol-related deaths.
In this section
- Policy reports
- Research
- Briefings
- Practical guides
- Alcohol Deaths Review Guidance
- Ministerial Foreword
- Introduction
- Phase One: Preparatory Work
- Phase Two: Establishing the Team
- Phase Three: Planning the Review
- Phase Four: Undertaking Research
- Phase Five: Preparing and Disseminating Findings
- Factsheets
- Consultations
- Manifesto
- Corporate documents
